
A 56yo female is brought to the ED after being pulled out of a house fire. EMS found patient unresponsive with pulse, in burning house. Patient was extricated from the house and on initial EMS evaluation patient was desaturating on room air. She was placed in nasal canula, but continued to have low oxygen saturation, and so was placed on 100% O2 via nonrebreather with improvement in oxygenation en route to ED. Patient subsequently awakened and complained burning sensation in her throat and shortness of breath. ED staff met EMS on arrival, and primary assessment by emergency physician was remarkable for soot on face, around mouth, and in nares and oropharynx, the rest of exposed skin appeared reddish in color. Lungs were clear to auscultation, through increased work of breathing was noted. Strong regular pulses were present. Patient was somnolent, but arousable, and able to answer questions appropriately, an no gross focal neurologic deficits were noted. Patient vital signs were notable for oxygen saturation of 96% on 100% oxygen via nonrebreather and otherwise unremarkable.
Emergency physicians were concerned for laryngeal edema and airway compromise due to airway burns, as evidenced by soot in and around airway. Additionally, the continued somnolence, increased work of breathing, and new high oxygen requirements all suggested impending airway disaster.
Patient was intubated via video Glidescope with RSI, and during the intubation, significant soot was noted in airway including down onto vocal cords.
Initial ABG with co-oximetry: pH 7.2, pCO2 in the 30s, carboxyhemoglobin 25.4%, The patient was begun on treatment for suspected cyanide poisoning along with carbon monoxide poisoning.
She was emergently transferred to a tertiary care facility with hyperbaric oxygen chamber
Inhalation injury
Definition: Inhalation injury is damage to the respiratory tract and/or lungs from heat, smoke or chemical irritants that enter the airway via inhalation. “Pulmonary complications following burns and inhalation injury are responsible for up to 77% of deaths after fires.” 5
Important historical features to note include: the type of exposure, the duration of exposure, and if patient was in enclosed space or lost of consciousness. Concerning physical exam findings for inhalation injury include: facial burns, singed nasal hair, soot in upper oropharynx, carbonaceous sputum, horsiness, stridor, tachypnea, decreased breath sounds, wheezing, rales, and rhonchi. Chest x-ray is usually unhelpful and normal after inhalation injuries, however if abnormal, indicates a more severe injury.
Upper airway injuries (above the vocal cords) are usually caused by direct thermal damage, and signs of injury include erythema, ulcerations, and edema. Patients may later develop increased secretions, obstructions, atelectasis, and impaired gas exchange. Deeper in the respiratory tract, chemicals in smoke damage the tracheobronchial tree leading to persistent coughs, wheezing, increased work of breathing and soot-containing airway secretions (melanoptysis). Chemicals from the smoke cause neuropeptide release creating reactive oxygen species and inflammation leading to cell damage, edema, and hypoxemia. Lung parenchymal injury can be delayed, but more severe injuries present sooner and correlate with decreased PaO2: FiO2. Injuries this deep impair oxygenation secondary to alveolar collapse, decreased surfactant, increased fibrin deposition, increased pneumonia risk, and increased blood flow to poorly ventilated bronchioles due to nitric oxide release.
Diagnosis: Direct airway exam, can get limited picture from nasopharyngoscopy or direct laryngoscopy, but the standard to confirm diagnosis of inhalation injury is fiberoptic bronchoscopy. Typical findings seen on bronchoscopy are mucosal erythema, edema, blisters, ulcers, bronchorrhea, fibrin casts and charring.5
Treatment: Secure the airway! If patient does not need immediate intubation, then apply 100% O2 via face mask with goal of >90% oxygen saturation. If there is concern for CO2 retention, can switch to bilevel positive airway pressure (BiPAP). In general, the emergency physician should have a low threshold for intubation. When intubating, try to use >7.5mm endotracheal tube (ETT) to facilitate bronchoscopy, but have smaller back up airways and alternatives ready, as swelling may limit the ability to pass larger tubes. Look for deep neck/face burns, oropharyngeal edema or blisters, respiratory distress. Edema can be delayed for 24-36 hours, so the astute clinician should have a low threshold to intubate early before significant swelling develops. Bottom line: if any question of airway compromise, intubate.
Consider calling Poison Control, if suspicion exists for toxic gas inhalation, as patients benefit from prompt administration of appropriate antidotes. Initially, use 100% O2 for carbon monoxide and cyanide toxicity, and hold weaning if on ventilator. Keep oxygen humidified to keep secretions thin. Bronchodilators and racemic epinephrine can be used for wheezing. To keep airways open and thin secretions can use n-acetycysteine or aerosolized heparin and mechanical means such as chest physiotherapy, suctioning, coughing, and early ambulation.
Special population Considerations
Pediatrics: The most common cause of severe morbidity and mortality in children is airway compromise. For this reason, there should be a lower threshold to intubate children with inhalation injuries. Use correct ETT sizing with back-ups on standby and verify that ETT is secure as children are more likely to displace ETT with deadly outcomes.
Elderly: Patients older than 65 have a mortality 6 times the national average.
Vent: no specific ventilator settings, attempt to limit TVs and plateau pressures to lowest tolerable.
“Mechanical ventilation of patients with inhalation injury should begin with low tidal volumes (6 to 8 mL/kg), adjusting them based upon the patient’s condition, compliance, airway resistance, and tolerance. There is no consensus on the optimal mode of mechanical ventilation, but if the patient develops acute respiratory distress syndrome, a lung-protective strategy should be used. Assessing readiness for extubation and daily weaning trials should be evaluated every morning, and the patient should be removed from mechanical ventilation as soon as he/she meets criteria.”1
Disposition of low risk patients: If, based on history and physical, the patient is judged to be at low risk for inhalation injury, monitor for 4-6 hours.
Long-term: Most patients do not suffer long term functional impairment. Patients that are more likely to have long term sequalae are those that had severe chemical bronchitis or nosocomial pneumonia at time of injury.
In addition to direct damage to respiratory tract by inhalation, toxic gases inhaled by patients can causes systemic effects. Assume carbon monoxide (CO) poisoning in inhalation injuries until normal carboxyhemoglobin level results.
Toxic Gases/systemic toxicity
Carbon Monoxide poisoning:
What it is: Odorless, tasteless, colorless gas with an affinity for hemoglobin more than 200 times that of oxygen. Incomplete hydrocarbon combustion forms carbon monoxide, and as a result, CO poisoning is seen most often with fire-related smoke inhalation. It is also commonly seen in winter and cold climates from exposure to poorly functioning heating systems. Methylene chloride (dichloromethane), a component of paint remover, when inhaled or ingested is metabolized to carbon monoxide in the absence of CO in air and can cause CO poisoning.
“Pulmonary-related complications following burns and inhalation injury are responsible for up to 77 percent of the deaths, most of which are related to carbon monoxide poisoning.” 1
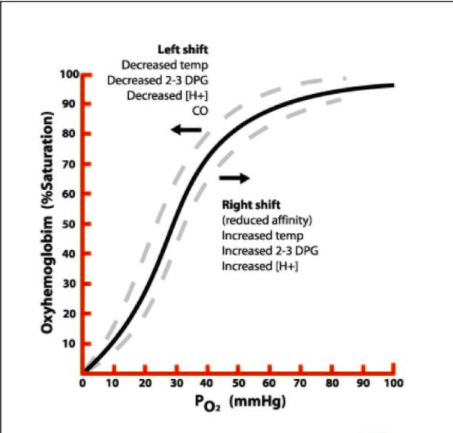
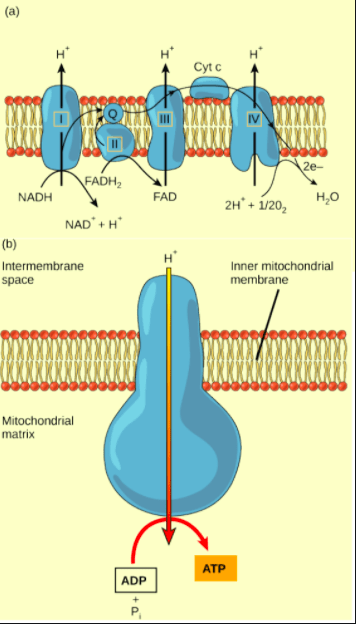
Pathophysiology: CO binds Hb better than oxygen, forming carboxyhemoglobin (COHb) and shifting oxyhemoglobin dissociation curve to the left, impairing oxygen delivery to tissues, CO also binds other molecules impairing oxidative phosphorylation in mitochondria leading to tissue hypoxia and myocardial stunning. Synergistic effects are seen with concomitant cyanide poisoning. The mechanism of development of delayed neurologic sequelae (DNS) is unclear, but the leading hypothesis involves CO causing lipid peroxidation. DNS can include cognitive deficits, personality changes, movement disorders, and focal neurologic deficits and typically occur within 20 days of poisoning.
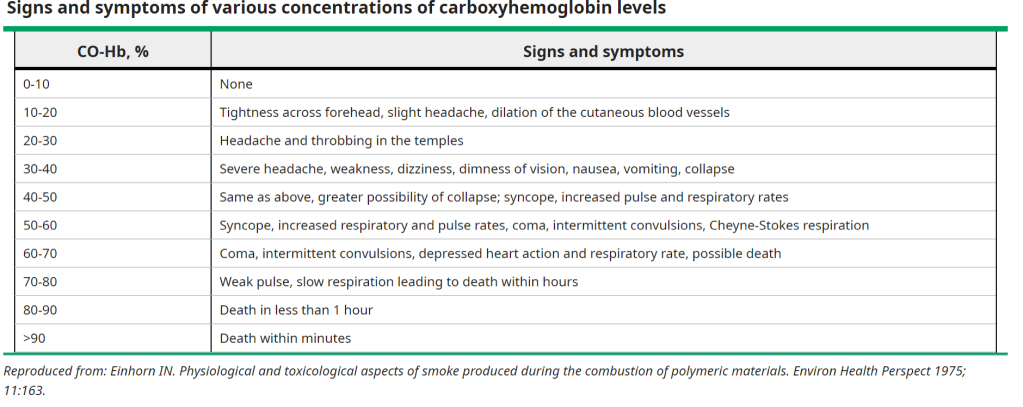
Signs and symptoms: Nonspecific, usually headache, nausea, malaise, dizziness. Can also cause altered mental status, loss of consciousness, myocardial infarction (MI), arrhythmias, pulmonary edema, lactic acidosis, seizures, and coma. While classically taught, cherry red skin and lips are not a sensitive sign for CO poisoning. ACUTE MI is COMMON among CO poisoning patients!!! Pediatric patients may present subtly, such as with increased fussiness and feeding difficulty.
4 Diagnosis: Have a high level of suspicion for carbon monoxide poisoning and treat based on history of the presenting illness and physical exam. Also, consider if multiple patients present with AMS, acidosis or coma. Standard pulse oximetry is NOT reliable as it cannot distinguish between COHb or oxyhemoglobin. A blood gas with Co-Oximetry is necessary. Order EKG, troponin if >65 years old, or with significant cardiac risk factors or chest pain. Consider CT head and additional labs (including cyanide level) if patient is altered. Brain imaging may show globus pallidus lesions with carbon monoxide poisoning.
At baseline nonsmokers should have <3% COHb, while smokers may have up to 10-15% COHb
Treatment: Remember the basics; first ABCs, close monitoring, intubate as needed (AMS/coma/airway compromise) and keep FiO2 100% for vented patients and 100% O2 via face mask/nonrebreather until asymptomatic for all others. The half-life of COHb decreases with increased oxygen inhalation. The actual levels of COHb are imprecise and do not need to be repeated. The only caveat to this is determining whether the patient would benefit from hyperbaric oxygen (HBO) treatment.
Hyperbaric oxygen candidates:
- HBO if CO level >25% ( >20% if pregnant)
- Loss of consciousness
- pH <7.1
- concern for end organ ischemia (chest pain, EKG changes, AMS).
HBO should be begun as quickly as possible, ideally within 6 hours. HBO decreases half-life of COHb to about 30 minutes, and studies suggest that it lowers short, and long term, mortality rates. Airway must be secure, and patient needs to be hemodynamically stable prior to transport/HBO treatment.
Consider empiric cyanide treatment with smoke inhalation.
Pediatrics: Children are managed the same as adults, however, they may need myringotomy with AOM due to increased pressure with HBO and possible tympanic membrane rupture, parental support in chamber if HBO, and extra care to keep infants warm. Caution in patients with ductal dependent cardiac lesions as increased oxygen levels can lead to ductus arteriosus closure and cardiopulmonary compromise.
Disposition: Most patients who have mild symptoms that resolve with oxygen can be safely discharged. Those with severe, or non-resolving symptoms or severe poisoning (>15% COHb or other ill effects) should be admitted to hospital. Make sure to screen for suicidal ideation or intentional CO poisoning. Most importantly, for patients being discharged, ensure that their home or work is no longer a source of CO poisoning.
Cyanide poisoning
Definition: Hydrogen cyanide is the gaseous form of cyanide; it is a colorless gas with the odor of bitter almonds. This toxic chemical is generated during the combustion of synthetic materials, wool, and silk. Cyanide toxicity is difficult to confirm initially due to its nonspecific symptoms and inability to measure cyanide levels soon enough to be clinically meaningful. Additionally, treatment should not be delayed until confirmatory levels as cyanide poisoning is rapidly lethal unless treated with an antidote, within minutes to hours. Consider cyanide poisoning after house fires in inhalation patients as well as in industrial (mining, electroplating, plastic manufacturing) workers and those with direct access to cyanide. Medical exposures include antineoplastic agent Amygdalin, and anti-hypertensive medication, Sodium nitroprusside. Pits/seeds of fruits such as cherry laurel and, plums are rare causes. Homicide/suicide by intentional ingestion of cyanide salts is also possible.
Initiate empiric treatment when patients present with concerning history of present illness and depressed levels of consciousness, cardiac arrest, or cardiac decompensation.
Pathophysiology: Cyanide is a mitochondrial toxin that by binding cytochrome oxidase a3, inhibits oxidative phosphorylation, forcing cells to switch to anaerobic metabolism to generate ATP. Anaerobic metabolism leads to lactic acidosis. Cyanide also inhibits antioxidants, leading to oxygen free-radicals, and affects neurotransmitters increasing the risk of seizures.
Cyanide neutralization most importantly involves a sulfur donor for the enzyme rhodanese via thiosulfate to allow rhodanese to convert cyanide to thiocyanate that is excreted in the urine. A minor cyanide neutralization pathway uses hydroxocobalamin, which combines with cyanide to form cyanocobalamin, which is excreted in urine. A small amount of unmetabolized cyanide is excreted via urine, sweat, and expiration.
Signs and symptoms: Depending on the cyanide compound and route of exposure the patient may have headache, anxiety, confusion, vertigo, metallic taste, cough, shortness of breath, vomiting, or abdominal pain. Physical exam initially shows hypertension and tachycardia with tachypnea but progresses to bradycardia, hypotension, and bradypnea. Cherry red skin/flushing is uncommon, cyanosis or dermatitis may be seen. Bitter almond or unusual odor can be smelled. Patients may have seizures and possibly coma as poisoning progresses. Later cyanide poisoning can cause renal failure, hepatic failure, rhabdomyolysis, and pulmonary edema.
Diagnosis: Labs show an elevated lactic acid, which closely correlates with severity of toxicity, thus trending can be used to monitor treatment progress. A normal serum lactate suggests an alternate diagnosis for the patient’s symptoms. Due to the elevated lactic acid, an anion gap metabolic acidosis is usually seen. An ABG with co-oximetry should be ordered on all inhalation injury patients and cyanide poisoning patients should be carefully evaluated for additional diagnoses like carbon monoxide poisoning or methemoglobinemia as they are frequently co-existing. Cyanide concentration level can confirm diagnosis, but levels are typically not available in a timely fashion and treatment should not be delayed to await the level.
Treatment: Secure airway! Intubation is usually required in cyanide poisoning. Administer supplemental oxygen regardless of pulse oximetry readings. Decontamination for dermal exposure, remove clothes, cleanse skin. Avoid rescue breaths due to rescuer exposure risk. Consider activated charcoal if ingested <1 hour with patent airway. Cyanide poisoning commonly presents along with CO poisoning. Symptomatic treatment may also be needed, such as IV fluids and vasopressors for hypotension and benzodiazepines for seizures.
Consider cyanide treatment when inhalation victim has 2 or more of the following: carbonaceous sputum, AMS, metabolic acidosis, lactic >8
First line Antidote: Hydroxocobalamin (CyanoKit) 5g IV over 15 minutes (70mg/kg in pediatric patients). (Can concomitantly administer sodium thiosulfate 25% solution 12.5g (50ml) IV (1.65ml/kg in pediatric patients)).
Second line Antidote: Cyanide Antidote Kit. Amyl Nitrite (inhaled) plus Sodium nitrite 3% (300mg IV). Followed by Sodium Thiosulfate 12.5g IV. (The goal of this treatment is to induce methemoglobinemia and then treat it).
Third line Antidote: If hydroxocobalamin and nitrites are either unavailable or contraindicated, can administer sodium thiosulfate in isolation.
Side effects: Hydroxocobalamin may causes temporary reddish discoloration of skin, plasma, urine and mucous membranes, headache, nausea, chest discomfort, decreased lymphocytes, bradycardia, hypertension, and interferes with further co-oximetry.
Treatment with amyl nitrite or sodium nitrite is contraindicated in cases of concomitant carbon monoxide poisoning as both shift oxygen dissociation curve left and cause tissue hypoxia that could be lethal. Avoid nitrites in pregnant women and severe hypotension.
Thiocyanate can cause psychosis, vomiting, and myalgias.
Pediatrics higher risk of cyanide poisoning, same treatment, dose 70mg/kg IV (max 5g).
Disposition: Admission and typically intubation.
Delayed symptoms of cyanide poisoning: “Survivors of severe cyanide poisoning may develop delayed-onset Parkinsonism or other neurologic sequelae. The basal ganglia are particularly sensitive to cyanide toxicity”3
Written by: Mary Skiffey, DO
Peer reviewed and edited by: Dylan Kellogg, MD
References
- Clardy, P. F., MD, Manaker, S., MD, PhD, & Perry, H., MD. (2019, December 18). Carbon monoxide poisoning. Retrieved March 5, 2021, from https://www.uptodate.com/contents/carbon-monoxide-poisoning?source=history
- Cydulka, R. K., Fitch, M. T., Joing, S., Wang, V. J., Cline, D., Ma, O. J., & Tintinalli, J. E. (2018). Tintinalli’s emergency medicine manual. New York: McGraw-Hill Medical.
- Desai, S., MD, & Su, M., MD, MPH. (2019, March 25). Cyanide poisoning. Retrieved February 25, 2021, from https://www.uptodate.com/contents/cyanide-poisoning?search=cyanide%20poisoning&source=search_result&selectedTitle=1~51&usage_type=default&display_rank=1#H87270019
- Einhorn, I N. “Physiological and toxicological aspects of smoke produced during the combustion of polymeric materials.” Environmental health perspectives vol. 11 (1975): 163-89. doi:10.1289/ehp.7511163
- Mlcak, R. P., PhD, MBA, RRT, FAARC. (2020, March 20). Inhalation injury from heat, smoke, or chemical irritants. Retrieved March 05, 2021, from https://www.uptodate.com/contents/inhalation-injury-from-heat-smoke-or-chemical-irritants?source=history

You must be logged in to post a comment.