
A 70 year old female presents for hypoxia and altered mental status. On arrival she is tachycardic to 120, febrile to 38.5, hypoxic to 86% on room air, and is normotensive. She appears ill and confused. She has diffuse rhonchi throughout all lung fields. She has no significant past medical history. A workup is obtained that shows bilateral opacities on chest x-ray and her CBC returns with a WBC count of 205k (prior WBC count normal in our system). She also has severe anemia and thrombocytopenia with a hgb of 4.7 and plts of 36. Potassium is 6.0 without EKG changes. Her lactic acid is 13.
Leukostasis
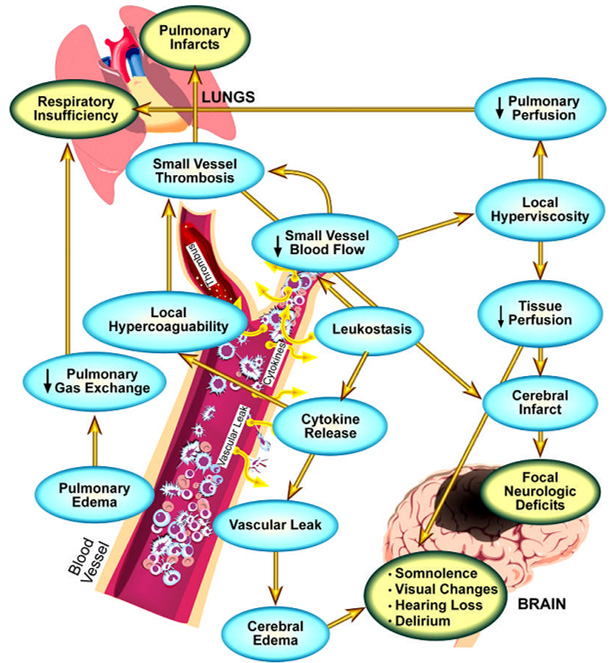
Leukostasis is a medical emergency most commonly seen in patients with leukemias in blast crisis. It is characterized by an elevated blast cell count and symptoms of decreased tissue perfusion. The pathophysiology of leukostasis is not well understood, but is thought to be secondary to inadequate delivery of oxygen to the body’s cells due to WBCs plugging the microvasculature. This is in contrast to hyperleukocytosis which is asymptomatic WBC elevation greater than 50-100k. Symptoms of leukostasis tend to start when counts reach greater than 100k.
Leukostasis is a medical emergency, with untreated patient mortality rates reaching 40 percent. It causes many complications including neurological sequela, respiratory failure, spontaneous tumor lysis syndrome, and DIC.
Presentation:
- Most common sign is fever
- Symptoms from “clogged” microvasculature:
- Neurological
- visual changes, headache, dizziness
- confusion, somnolence, coma
- patients can develop strokes from hyperviscosity
- Pulmonary
- dyspnea and hypoxia with or without diffuse interstitial or alveolar infiltrates on imaging studies
- Patients may require mechanical ventilation for respiratory failure
- Multi-organ failure
- myocardial ischemia and right ventricular overload, renal failure, acute limb ischemia and bowel infarction are possibilities
- Neurological
Labs:
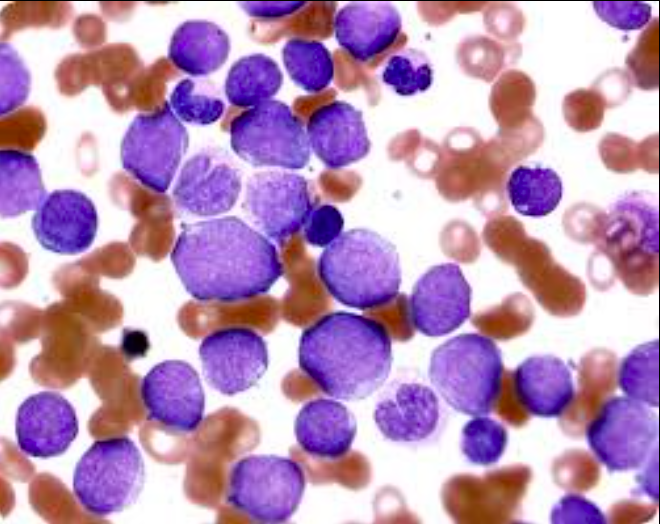
- CBC tends to have WBC greater than 100k with blasts seen on peripheral smear.
- Decreased PaO2
- ABG Measurements for arterial pO2 have shown to be falsely decreased in patients with hyperleuckocytosis
- pulse oximetry should be used to more accurately assess pO2 levels of a patient suspected to be suffering from leukocytosis
- Platelets may be inaccurate on CBC (fragments of blast cells can be mistakenly labeled as platelets). CBC needs to be manually reviewed by peripheral smear.
- Serum potassium levels may be artificially elevated on blood work. However, potassium may also be elevated do to spontaneous tumor lysis syndrome.
- Elevated coagulation studies (PT/PTT), increased d-dimer, low fibrinogen may be found in patients who develop DIC.
- Elevated uric acid, potassium, and phosphate as well as low calcium may be seen in patients who develop spontaneous tumor lysis syndrome.
Diagnosis:
Diagnosis is clinical when a patient presents with a WBC greater than 100k with signs of end organ dysfunction. Most commonly patients present with neurological complications and respiratory failure. It is possible to develop leukostasis at counts below this number and so a high degree of clinical suspicion needs to be maintained.
- Patients need a CXR to look for opacities
- Patients should have DIC considered and worked up
- Tumor lysis syndrome should be considered and worked up as this can happen spontaneously and not from chemotherapy
- End organ dysfunction needs to be considered (checking renal and hepatic function) including myocardial ischemia
- Lactate needs to be sent given tissue hypoxia
Treatment:
- Leukostasis is a medical emergency and prompt transfer to a center capable of chemotherapy and possible leukapheresis is needed emergently. Deterioration can happen at any time and rapidly.
- Chemotherapy
- Emergent induction chemotherapy can help reduce the WBC count as well as destroy leukemia cells
- Emergent heme/onc consultation is needed
- Leukapheresis
- Although controversial, heme/onc should be consulted and rapid transfer should be arranged for possible emergent leukapheresis in leukostasis
- Blood product transfusion
- Leukostasis can be worsened by transfusions, and if possible transfusions should be withheld as they can increase blood viscosity.
- If needed, transfusions should be performed very slowly.
- Of note, platelet transfusions need to be performed at a higher than normal threshold (30k rather than 10k) as the spontaneous bleeding rate is higher especially during periods of reperfusion
- Volume status
- Patients can be very sensitive to changes in volume status. Although fluid resuscitation can help renal failure and tumor lysis syndrome, it can also precipitate or worsen pulmonary complications.
- Resuscitate to maintain urine output and blood pressure but do not overhydrate.
- Supportive care for DIC and TLS.
- Supportive care for end organ dysfunction including intubation for respiratory failure if needed.
Case conclusion
The patient remained critically ill with a significant lactic acidosis, diffuse alveolar opacities on CXR complicated by hypoxic respiratory failure, and multiple signs of end organ dysfunction including renal failure and confusion. A quaternary care center was consulted and the patient was emergently transferred for induction chemotherapy and possible leukapheresis. After discussion with heme/onc at the receiving facility, transfusion was withheld. The patient did not develop DIC or TLS prior to transfer and did not require intubation.
Take home points:
- Leukostasis is a true medical emergency and requires emergent consultation and transfer for possible induction chemotherapy and leukapheresis.
- Patients can develop multisystem organ failure, however the most common complications are respiratory failure with bilateral opacities on CXR and neurological complications including confusion, somnolence, and coma.
- Beware of TLS and DIC.
- Be careful not to overhydrate with IV fluids.
- Avoid transfusions if possible as they can worsen symptoms.
- Patients can decompensate rapidly and at any time.

Nice summaation. Sounds like a complicated case.
LikeLike