History of Presenting Illness
An 81 year old male presented to the Emergency Department with chief complaint of low blood pressure and elevated blood sugars. This patient had a medical history significant for hypertension and hyperlipidemia. This patient is highly functional at his age up until about one week ago. He is able to ambulate independently, can drive himself and takes care of his own finances. Patient reported one week ago he began experiencing fatigue, generalized weakness, exertional shortness of breath as well as chills. He was seen in the Emergency Department at that point and chest xray, blood work and urine analysis were performed. His work up was unremarkable and patient was discharged. He continued to have similar symptoms for the rest of the week and then represented to the Emergency Department. On physical exam of the abdomen, a circumferential target lesion was noted. EKG was performed which showed a first degree AV block which was new in comparison to prior EKGs. Patient stated he had gone hunting 3 weeks prior to current presentation and did not recall any tick bites. In fact, patient had not even known about a rash until pointed out by the provider. Patient was admitted to the inpatient service with a diagnosis of Lyme Carditis and started on antibiotics.

Introduction
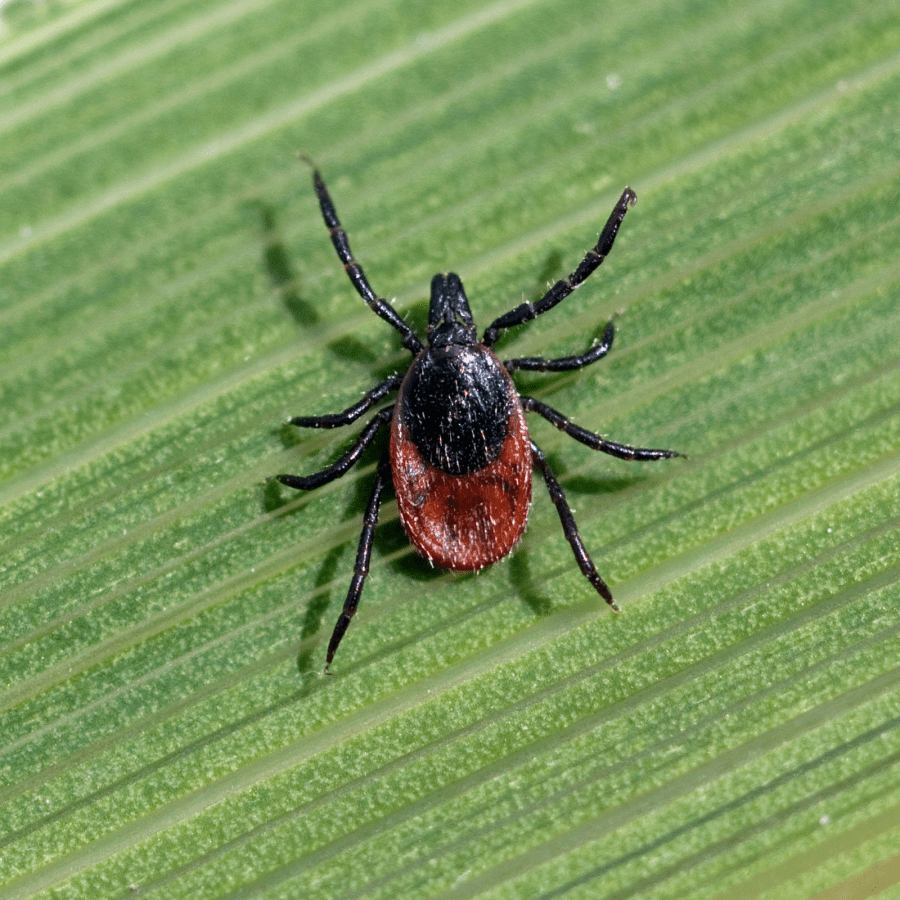
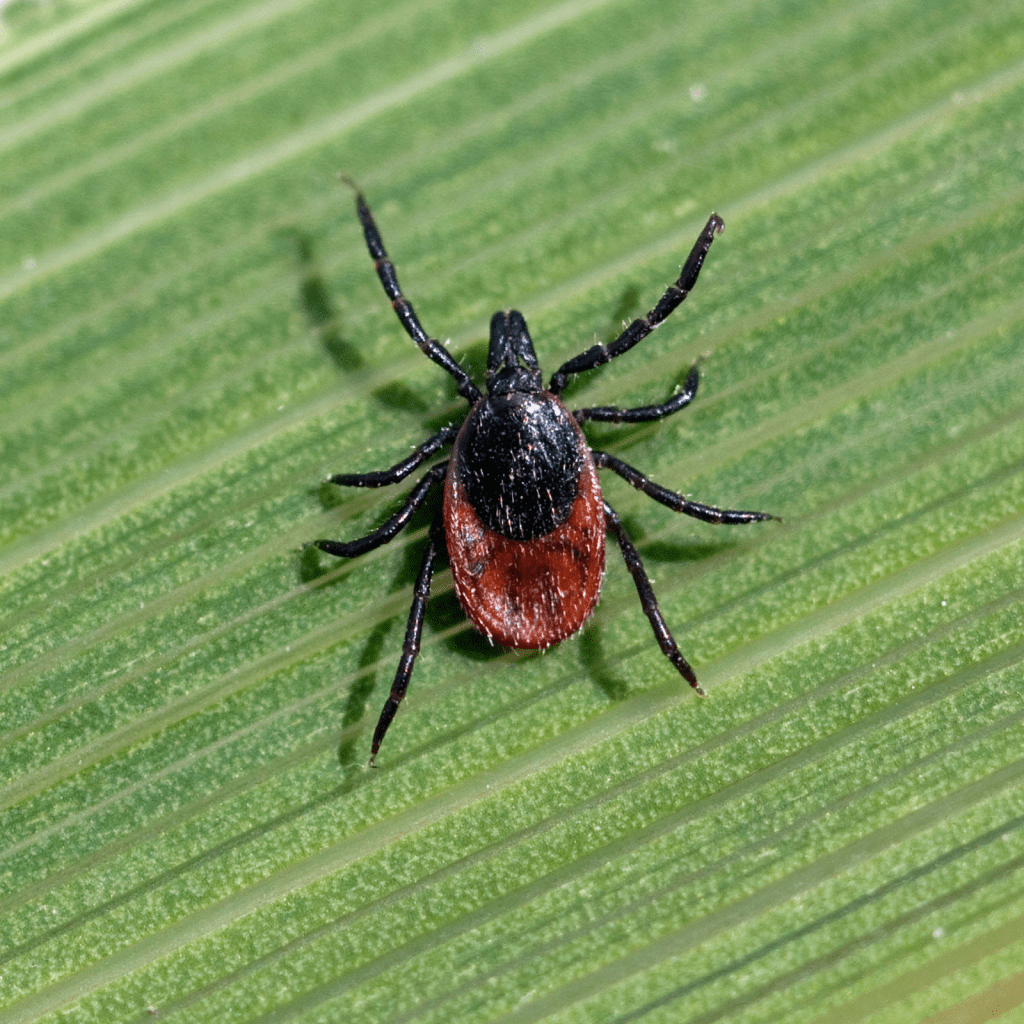
Lyme disease is the most common tick borne illness in the United States. It is caused by the spirochete Borrelia burgdoferi. The natural reservoir are mice, chipmunks, and other small mammals. The vector is the Ixodes tick. Lyme disease is most diagnosed between March and October with 95% of cases identified in the Northeast, mid-Atlantic, and Midwest states.
Clinical manifestations of Lyme disease occur in varying stages. The first phase is the early localized infection. This is characterized by the target lesion rash called erythema migrans. You may also have constitutional symptoms as well. The second stage, called acute disseminated infection, presents with neurological and cardiac manifestations typically 3-5 weeks later. Neurological infection includes Bell Palsy, meningoencephalitis. Cardiac manifestations include AV blocks. The last state, called Late Lyme disease predominantly includes neurologic and arthritic manifestations.
Most cases of Lyme carditis occur between June and December. Symptoms develop 4 days to up to 7 months following initial symptomology with a median of 21 days. The degree of AV block is fluctuating ranging from first degree to second degree to complete and back to first degree. Cases of endocarditis and myopericarditis have also been reported.
Evaluation
- EKG
- First Degree- fixed prolongation of the PR interval >200 milliseconds
- Second Degree (Mobitz 1)- progressive prolongation of PR interval followed by a nonconductive P wave
- Second Degree (Mobitz 2)- unchanged PR interval followed by a single non conducted P wave.
- Third degree- dissociation between P wave and QRS complexes.
- CXR – may show bilateral infiltrates or pleural effusions.
- ELISA to detect the presence of IgM or IgG. If present, confirm with Western blot.
Management
- For mild to moderate disease, oral amoxicillin or doxycycline for 14-21 days
- For severe disease- require hospitalization for IV antibiotics. Typical Ceftriaxone or Cefotaxime.
- Inpatient admission criteria
- Presence of syncope, dyspnea or chest pain
- AV Block of the second or third degree
- AV Block of first degree with PR interval greater than or equal to 300
- Treatment continues until resolution of conduction abnormalities and can transition to oral antibiotics.
- Temporary pacemaker placement may be required for high degree AV blocks or hemodynamic instability.
Deterrence
If traveling to endemic areas, minimizing the contact with tick can be achieved by:
- Wearing protective clothing
- Repellent application [such as permethrin or N, N-diethyl-meta-toluamide (DEET)] to clothing
- A thorough check and removal of ticks with the use of tweezers daily.
Antibiotic prophylaxis with oral doxycycline 200 mg is the recommended course for individuals with tick attachment for at least 36 hours.
Written by: Shyamal S Patel, MD
Reviewed by: Stevley Koshy, MD
References Uptodate ,Pubmed
