
46 year old male presents to the Emergency Room after eating a peanut, face swollen with inspiratory stridor. EMS reports being unable to intubate with the patient currently having a saturation of 78% on 100% CPAP. You take a look with your laryngoscope and see edema with no sign of vocal cords. The patient becomes bradycardic and goes into asystole. Cardiac arrest secondary to hypoxia while being unable to intubate or ventilate. Which means one thing.
In more than 50% of cricothyrotomies the indication was trauma. However the scenarios that may necessitate a surgical airway include airway obstruction, hemorrhage or anatomical abnormalities preventing adequate oxygenation from the upper airway including anaphylaxis and edema.
Albeit rare, a cricothyrotomy is defined as a surgical airway in the presence of not being able to intubate, ventilate and a patient is in severe respiratory distress. In a review of the different methods, the idea is the same. Bypass the oropharynx, and create an airway
It’s important to remember that in a can’t intubate can’t oxygenate scenario, extraglottic airway devices may be attempted, or placed while a cricothyrotomy is attempted.
Cricothyroidotomy
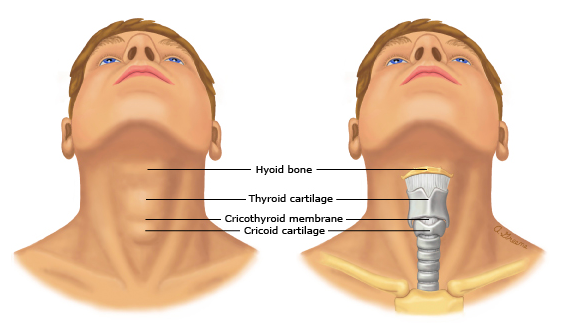
Perhaps the most important part of performing a cricothyrotomy is a well versed knowledge of the anterior anatomy of the neck.
To begin, extend the patient’s neck and palpate the laryngeal prominence. This is the superior portion of the tracheal cartilage to which palpation to the inferior portion leads to the cricothyroid membrane and then cricoid cartilage. It is here in which different techniques may be used to secure a patient’s airway.

Scapel-Finger-Bougie
Standing to your dominant hand’s side of the patient, use your non-dominant hand to immobilize the larynx by holding the tracheal cartilage. For example, a right handed provider should be on the right side of the patient, immobilizing the trachea with their left hand.
Palpate down to the cricoid cartilage (inferior to cricothyroid membrane), and create 4 cm incision vertically.

From here, blunt dissect to the cricothyroid membrane and create a horizontal stab incision through the membrane1,5. Hold this position in the trachea with a finger, and advance a bougie into the trachea to the carina. Once advanced, a 6 mm tracheal tube may be advanced over bougie 6 cm into trachea. An endotracheal tube may serve as a substitute in the event of lacking tracheal tubes.
Remove bougie, and secure tracheal tube. Placement may be confirmed with capnography and chest x-ray.

Rapid four step technique
Standing at the head of the bed, palpate the cricothyroid membrane. Create a 3 cm incision through skin, tissue and cricothyroid membrane. Place a tracheal hook into the cricoid cartilage, and while continuing to keep the larynx stable, insert a tracheostomy tube as discussed previously. A bougie may also be utilized, and was shown in a small randomized study to increase speed of procedure.

Seldinger Technique
Often found in commercial kits, this technique includes using an introducer needle with a syringe halfway filled with saline solution. As gentle pressure is applied to the cricothyroid membrane at a 45 degree angle.
Bubbles should appear when the needle has entered the airway. Remove syringe and needle, guiding the guidewire into the catheter in place. Alongside the guidewire, a 1.5 cm incision is made with a scalpel and dilator/catheter unit may be placed and secured.

Traditional technique
Similar to previous, stand to your dominant hand’s side of the patient. Immobilize the larynx with your non dominant hand. Palpate the cricothyroid membrane and make a 4 cm vertical incision overlying the membrane. Cut the membrane 3 cm horizontally and insert the tracheal hook under the thyroid cartilage.
Insert trousseau dilator and enlarge incision vertically. Tracheostomy tube may then be placed and secured with the obturator removed.

Needle Cricothyroidotomy
Recommended for children up to 10-12 years old as surgical airway has potential to damage larynx due to size and diameter of trachea.
Similar to seldinger technique, a needle is inserted into trachea until bubbles are visualized, at which point catheter remains in trachea and is connected to 3-0 tube connector or 3 ml

Of note, a 3 ml syringe may act as an adapter for a 7.5 mm endotracheal tube, or a 3.0 mm endotracheal tube may be inserted directly into the catheter hub.

Contraindications
Although there are no absolute contraindications, a relative contraindication includes fracture or transection of larynx, bleeding disorders, as well as children <81,4. This is due to the narrowest portion of a pediatric airway being the cricoid ring. As a child’s tracheal diameter is smaller than adults, the development of a supraglottic stenosis will significantly impair air flow1.
Special Considerations
Recent literature, Austin (2020), has noted the utility of using a point of care ultrasound (POCUS) with consideration of identifying airway structure. Although the primary modality for identifying cricothyroid membrane remains by palpation, a randomized study in 2018 noted an 81% success rate to identifying cricothyroid membrane which is a 10x improvement from palpation7. Bedside ultrasound has also showed merit in confirming ET tube placement with a sensitivity of 98.7% and a specificity of 91.1%, with an average time of 13 seconds for confirmation8. Identification of thyroid cartilage, cricoid cartilage and cricothyroid membrane should be performed and marked prior to induction of patient.
Complications
Complications are dependent on several factors including location of procedure and level of training. These include:
- Laceration to thyroid cartilage
- Perforation of posterior trachea
- Extratracheal placement of tube
Discussion
Although rare, current recommendations are for clinicians responsible for airway management to be competent in at least one technique which includes review of anatomy, procedural steps, and supplies available in the Emergency Department. Of note, most literature appears to favor the use of a bougie once a tract to the trachea has been formed with higher rates of success and speed3. Above all, continuous review of rare procedures and simulation practice are necessary for they inevitably become required.
Take Home Points
- Continuous review of anatomy as well as competency in cricothyrotomy technique is a necessity for all providers responsible for securing an airway
- The use of a bougie once the trachea has been accessed has been shown to improve success rates and speed to completion.
- This procedure is tactile and is largely aided by stabilizing the larynx with the non-dominant hand
- Familiarize yourself with the equipment available in your Emergency Department.
Written by: Hakkam Zaghmout, MD
Peer reviewed and edited by: Michael Witt, MD
References
- Sakles, John C. “Emergency cricothyrotomy.” Uptodate, Oct. 2020, https://www.uptodate.com/contents/emergency-cricothyrotomy-cricothyroidotomy?search=cricothyrotomy&source=search_result&selectedTitle=1~55&usage_type=default&display_rank=1#H40058161.
- https://journals.lww.com/em-news/blog/PhotographED/pages/post.aspx?PostID=540
- Hill C, Reardon R, Joing S, Falvey D, Miner J. Cricothyrotomy technique using gum elastic bougie is faster than standard technique: a study of emergency medicine residents and medical students in an animal lab. Acad Emerg Med. 2010 Jun;17(6):666-9. doi: 10.1111/j.1553-2712.2010.00753.x. Epub 2010 May 14. PMID: 20491685.
- Schroeder AA. Cricothyroidotomy: when, why, and why not? Am J Otolaryngol. 2000 May-Jun;21(3):195-201. doi: 10.1016/s0196-0709(00)85024-3. PMID: 10834555
- Murray, Keith. “Chapter 30: Surgical Airways.” Tintinalli’s Emergency Medicine: a Comprehensive Study Guide, by David Cline et al., McGraw-Hill Education, 2020, pp. 194–200.
- Hebert RB, Thomas D. Cricothyrotomy and percutaneous translaryngeal ventilation. In: Roberts JR, Custalow CB, Thomsen TW, et al., eds. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. 7th ed. Philadelphia, PA: Elsevier; 2019:(Ch) 6.
- Siddiqui N, Yu E, Boulis S, You-Ten KE. Ultrasound is superior to palpation in identifying the cricothyroid membrane in subjects with poorly defined neck landmarks: a randomized clinical trial. Anesthesiology. 2018;129(6):1132-1139.
- Gottlieb M, Holladay D, Peksa GD. Ultrasonography for the confirmation of endotracheal tube intubation: a systematic review and meta-analysis. Ann Emerg Med. 2018;72(6):627-636.
