An 85 y.o f with a hx of DM and HTN presents with chest pain that awoke her from sleep at 5am. She described the pain as substernal with some mild radiation to the back. It was associated with nausea and lightheadedness. On exam, the patient appeared to be in moderate distress from her pain, clutching her chest. Her lungs were clear, there were no murmurs, and she had symmetric bilateral pulses. No signs of DVT or fluid overload on exam.
An EKG was obtained:
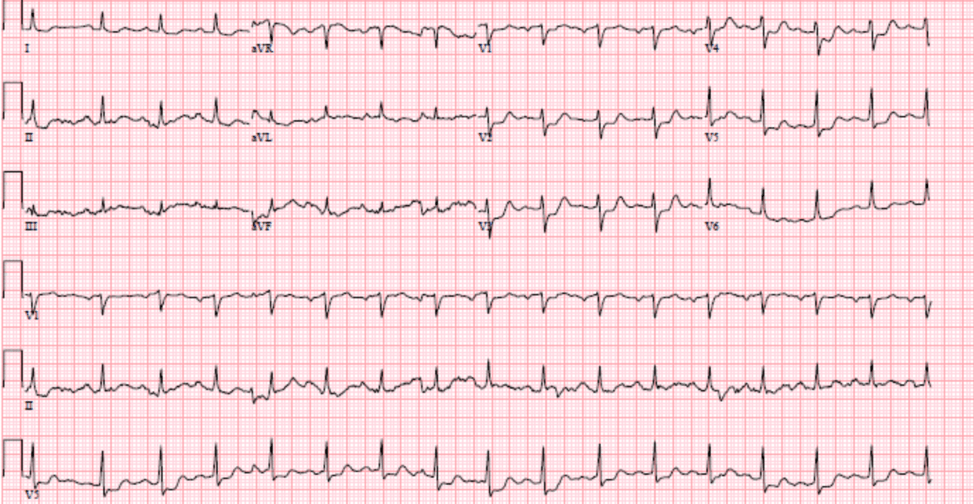
What is your interpretation of this EKG and what would be your next step?
The EKG shows ST depressions in V1 – V3. There are no ST elevations or T wave inversions. The EKG findings are concerning for a posterior MI.
We attempted to obtain a posterior EKG however the patient was in too much distress and we could not obtain an adequate one. The cath lab was activated and while awaiting cath, the patient’s troponin returned at 4,000.
Cath findings:
- 100% occlusion in proximal circumflex
- 85% occlusion in proximal 1st obtuse marginal
- 75% stenosis at the ostium of L circumflex
Stents were placed in all 3 vessels.
Posterior MI
- Posterior infarction accompanies 15-20% of STEMI’s (usually coincide with inferior or lateral MI’s)
- Due to no ST elevation, these are frequently missed.
Spotting a Posterior MI
- Horizontal ST- depressions in anteroseptal leads (V1-V3)
- Why do these changes occur in this pattern?
- The anteroseptal leads are directed from the anterior precordium towards the internal surface of the posterior myocardium. Because posterior electrical activity is recorded from the anterior side of the heart, the typical injury pattern of ST elevation and Q waves becomes inverted
- What do you do if you see these changes?
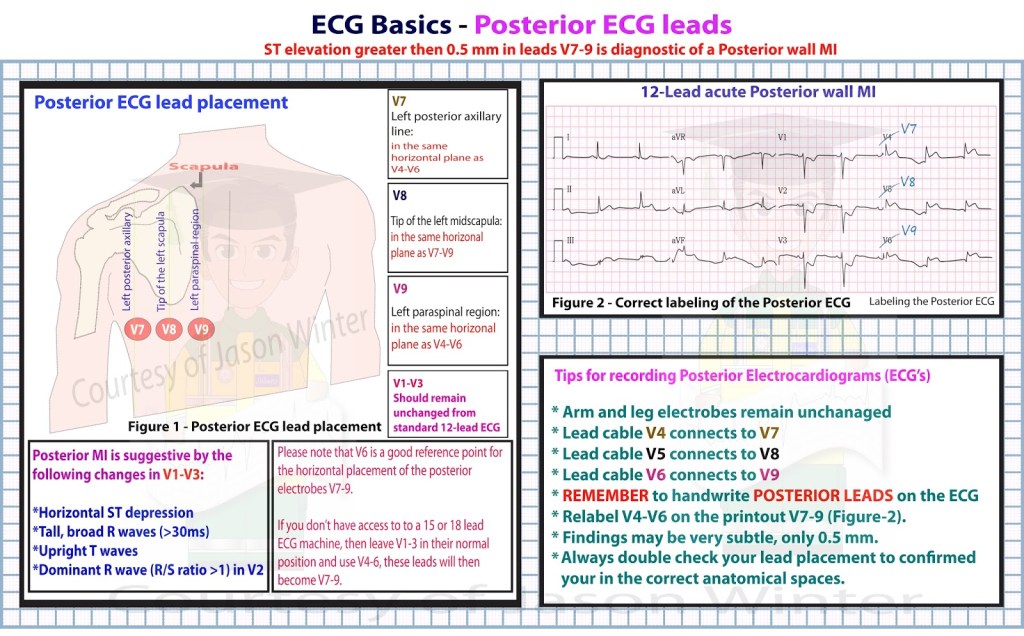
- Posterior EKG
What’s a posterior EKG?
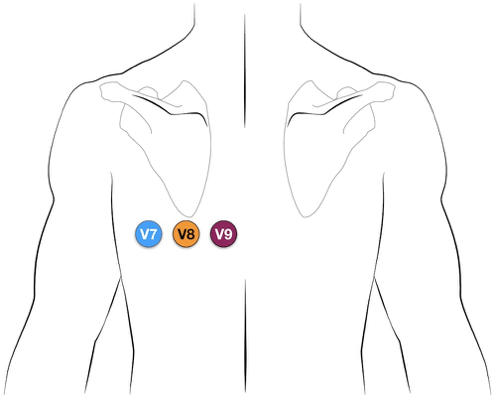
Three EKG leads are moved to the back (V4, V5, V6 are moved to the back) and are placed as shown above. These are re-labeled V7, V8, and V9. If there is posterior myocardial involvement, you should expect to see ST elevations in V7, V8, and V9.
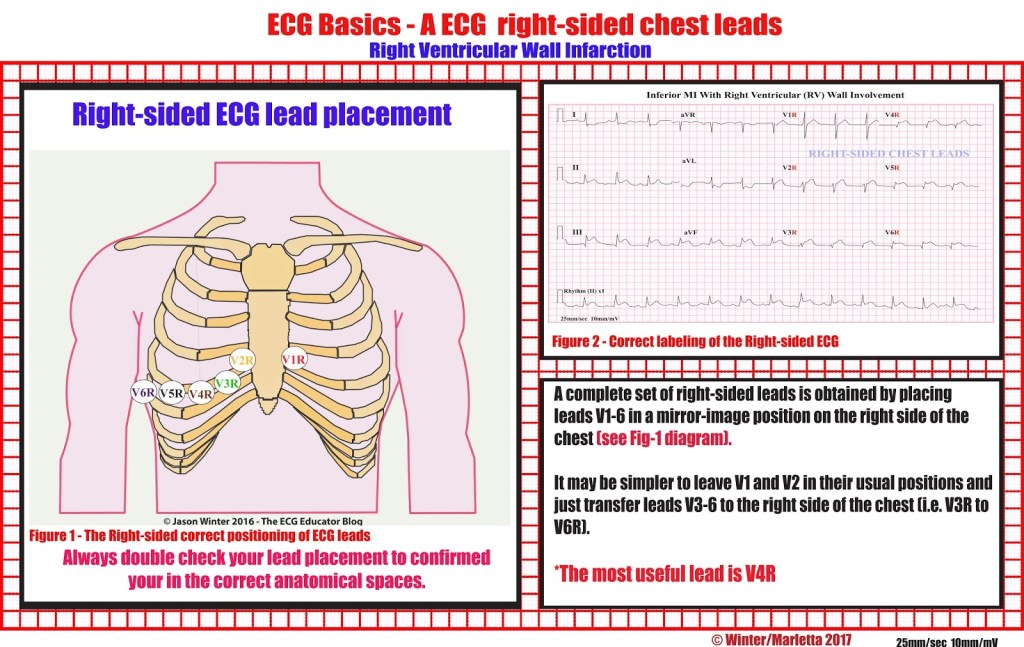
Right Sided EKG’s
These are not the same as right sided EKG’s. A right sided EKG is performed like this:
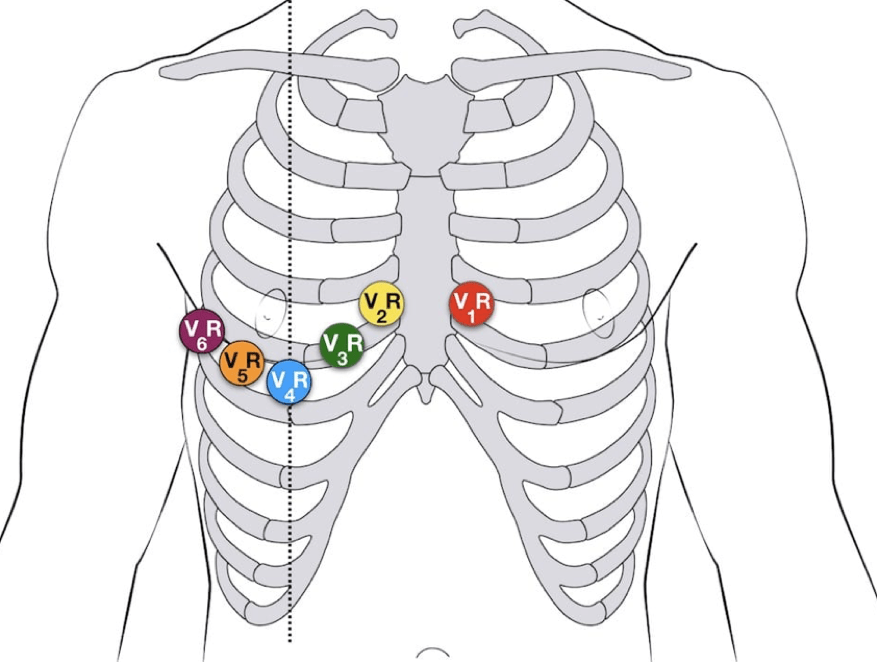
A right sided EKG is used when you have an inferior MI to see if there is right heart involvement. You would want to know this because inferior MI’s with right heart involvement are especially preload dependent and tend to have profound hypotension when given nitroglycerin.
If you see elevations in your new/right sided V1-V6 that you didn’t see prior, it indicates that there is right heart involvement.
Take Home Points:
- Posterior MI’s are a STEMI equivalent and many times will not have elevations on an EKG.
- Look for ST depressions in V1-V3 and consider obtaining a posterior EKG.
- Posterior MI’s are STEMI equivalents and warrant cath lab activation.
Author:
Sumyyah Yousufi, DO
Peer Reviewed and Edited By:
Timothy Stokes, MD

You must be logged in to post a comment.