
An 84 y.o f with no hx of heart or lung disease presents for altered mental status. Per care facility, the patient was in her normal state of health until the day of evaluation when they went to check on her and found her altered. EMS found her hypoxic to 70% and placed her on 6L NC. On arrival, pt was alert but altered. Her lungs are clear. She does not appear volume overloaded. She is not febrile or hypotensive. Her HR is 110.
Bedside ultrasound was performed:
In video 1, you can see a hyperdynamic left ventricle. Although you can not tell the size of the right ventricle on the parasternal long, you can see on that the right ventricle dose not seem to have as much motion/squeeze as it normally does. This is indicative of a reduced right ventricular ejection fraction.
In Video 2, although there is not a definitive D sign throughout the entire cardiac cycle, you can actually see signs of right ventricular overload with an intermittent D sign. Watch the septum closely during diastole. You will see that rather than being perfectly round like the donut that it typically looks like in a parasternal short axis, it temporarily becomes a D/bowed in and looks like someone is jumping on a trampoline. This is a sign of right heart strain.

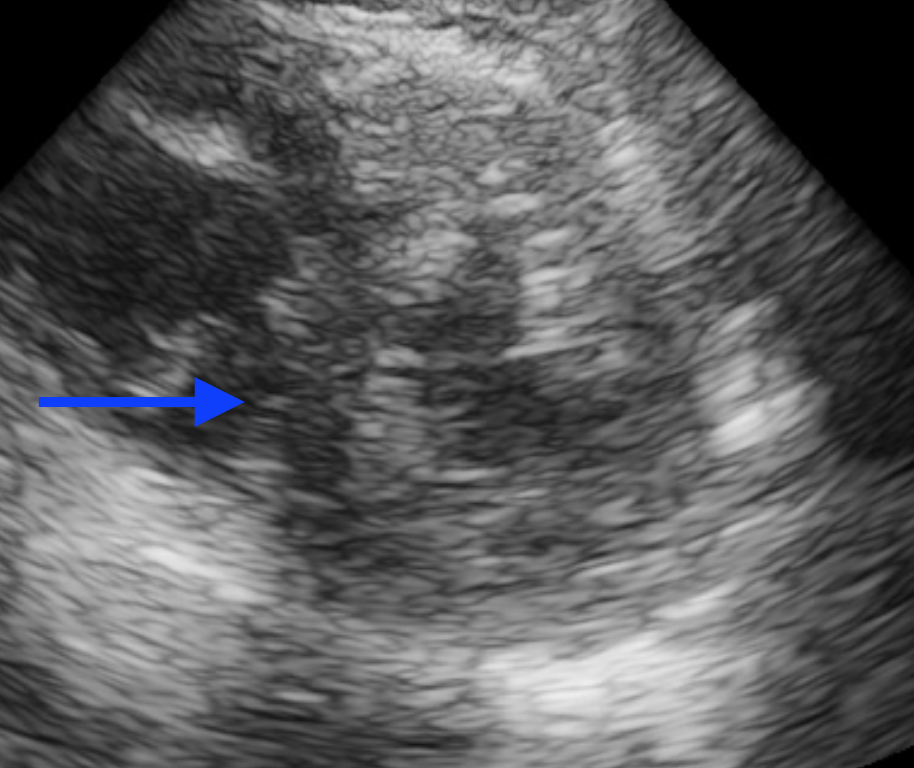
In video 3, you can see the reduced squeeze of the RV and you can also see that the RV is approaching the size of the LV. Normally, the RV should be smaller than the LV. If on an apical 4 chamber view your RV is as large as or larger than your LV, you should be concerned about right heart strain. There is also deviation of the septum on the apical 4 chamber view into the LV which is abnormal and from the RV pressure overload.
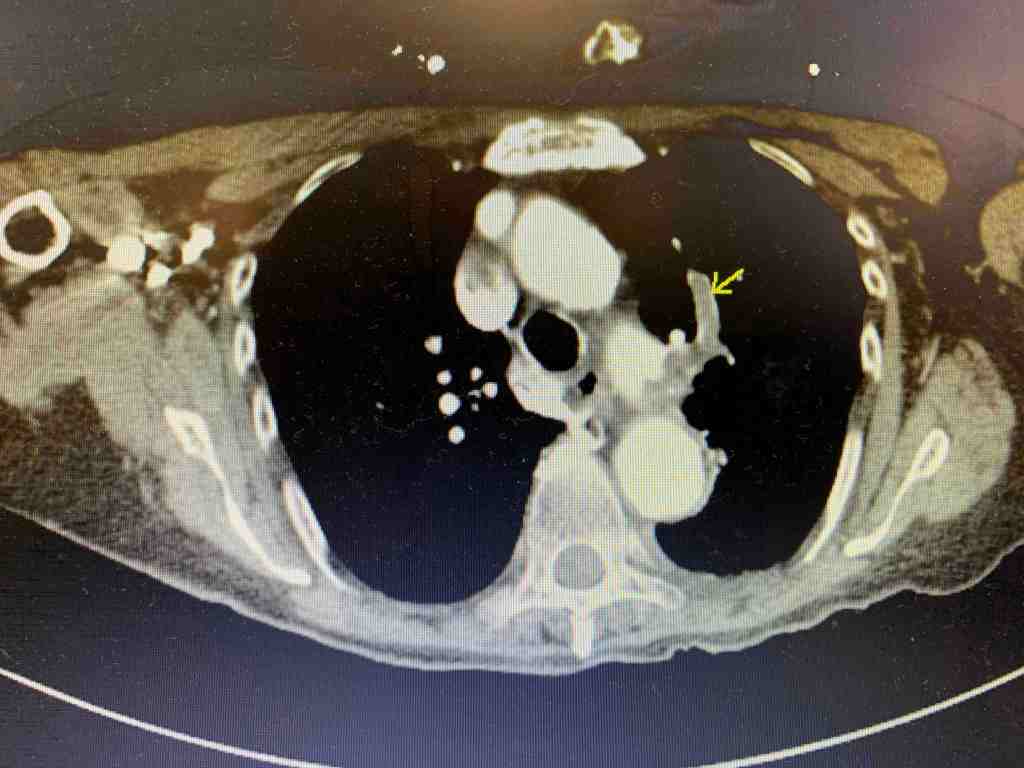
Given the above bedside ultrasound, there was concern for PE as the cause of the patient’s hypoxia. CTA was obtained and showed bilateral segmental PE’s.

The patient was started on anticoagulation and admitted. Her blood pressure remained stable but she continued to require 6L of O2 by NC and her troponin continued to rise. Cardiology based echo showed:

Take Home Points:
- In an unstable patient, bring the ultrasound to bedside to narrow your differential and guide your resuscitation
- Don’t neglect the RV – decreased function, enlarged right heart, and a D sign can mean right heart strain and narrow your differential to pathologies that cause right heart strain
- Hypoxia, clear lungs, and right heart strain = PE until proven otherwise
