It’s a little after midnight when a middle aged male walks into the ED complaining of chest pain. The triage nurse immediately grabs you because she’s concerned about the way the patient looks.
You walk into the room and see a man with mild diaphoresis and stable vitals. He mentions he started having pain in both of his shoulders about an hour prior to arrival. The pain slowly migrated to the middle of his chest and then to the left jaw. Other than a prior history of malignancy he denies any other medical problems including no history of coronary artery disease, diabetes, or blood clots.
You order the typical cardiac work up along with ASA and NTG.
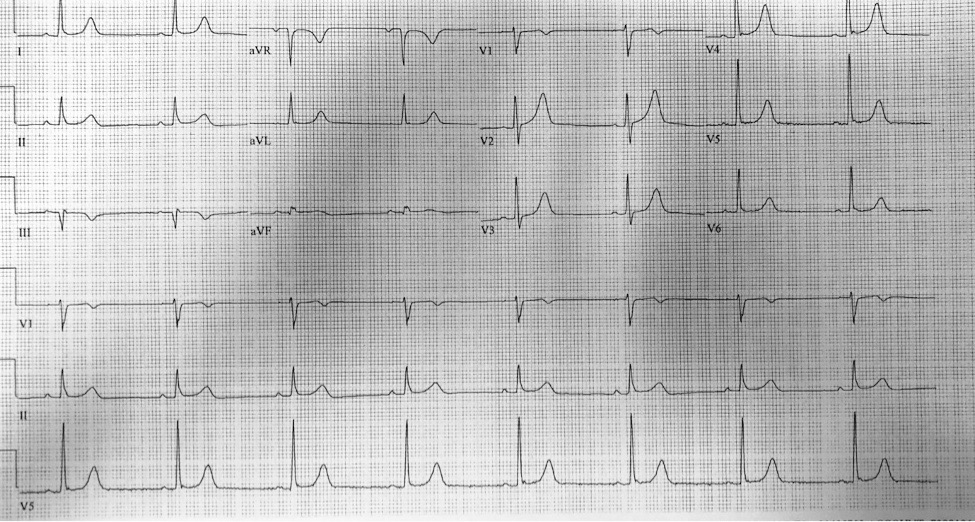
Initial EKG:

In the inferior leads there is subtle submillimeter ST segment elevation. There is starting to be the loss of a concave shape ST segment in III and aVF. There is no reciprocal change.
The decision was made to perform serial EKGs and discuss the EKG with interventional cardiology. Interventional cardiology stated there was no need to activate the cath lab immediately, but they would intervene if the pain persisted or progressed.
By that point the patient’s chest pain had improved and the diaphoresis had resolved. 2 more EKGs were performed 15 minutes apart from each other:
EKG #2:

EKG #3:
His repeat EKGs were essentially unchanged from prior and the patient remained chest pain free. The patient’s initial troponin came back at <0.03.
Almost 2 hours in to his ED visit his chest pain returned along with the diaphoresis. A fourth EKG was ordered which you can see below:

This EKG showed subtle yet progressive elevation in III as well as the beginnings of ST depressions and reciprocal change starting in aVL
Interventional cardiology was paged again regarding the concerning EKG changes and change to his pain. The decision was made to take the patient for an emergent cath which showed a 100% proximal RCA and 85% mid RCA occlusion, both of which were stented. His next troponin came back at 17.5.
Take Home Points
- Lead aVL can sometimes be the only/first sign of reciprocal change developing in ACS
- Early signs of STEMI can sometimes just be ST segment flattening or loss of the concave shape of the ST segment.
- An early STEMI can have a negative initial troponin.
- Remember to take advantage of serial EKGs. If the EKG is concerning, the story is good, and/or there’s a change in pain get another EKG!
